

An estimated 20,000 people suffer from Crohn’s disease (CD) in New Zealand, a type of inflammatory bowel disease, and it’s becoming increasingly prevalent here and around the world.
While treatments include immunosuppressive medications, dietary changes and surgery, the underlying cause of the disease remains a matter of debate amongst scientists and clinicians. However, research led by Awanui Labs pathologist Andrew Tie and Otakaro Pathways microbiological scientist John Aitken is challenging the rationale.
Their study has identified a type of mycobacterium they believe is the underlying cause of Crohn’s disease, which requires further examination within the science and health community.
The hypothesis
“Our research builds on over 40 years of Crohn’s disease research exploring the biology of Mycobacterium avium subspecies paratuberculosis (MAP) as both a cause of Johne’s disease – a bowel illness found in animals – and Crohn’s disease in humans,” says Dr Tie.
“We accept this is not conclusive proof but taking the documented pathological similarities between Johne’s disease and Crohn’s disease into account, we consider MAP causes both diseases, in differing forms of the bacterium.
“The collaboration between Awanui Labs and Otakaro Pathways was the opportunity to directly address this connection.”
Methodology for the study
To investigate this hypothesis, the study analysed tissue colon samples from eighteen patients diagnosed with Crohn’s disease in Wellington Hospital, between 2015 and 2019.
These samples were compared with samples from fifteen cases of normal colon, and positive animal tissue samples for Johne’s disease, which formed another control group.
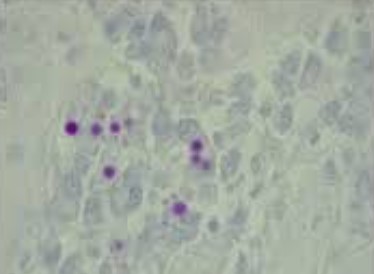
Dr Tie says when MAP exists in humans, the bacterial cells are no longer protected by an outer wall and reduced to a membrane. These are known as cell-wall deficient mycobacteria (CWDM) which also swell osmotically and change from a rod-shaped bacterium to a sphere.
“We used a modified Ziehl-Neelsen stain, a laboratory technique used to detect mycobacteria, because CWDM can be difficult to detect using conventional stains when the cell wall is absent.
“While one modification of the ZN stain damaged the tissue samples, the second revealed the spherical organisms, like those previously observed by John in cultures from patients with Crohn’s disease.”
Results point to an underlying cause
Dr Tie says CWDM organisms were detected in all eighteen samples from patients with Crohn’s disease when the team used the decolourising agent with more concentrated acid alcohol in the Ziehl Neelsen stain.
“The results showed there was a variation in the size and clustering of the organisms, although CWDM were not detected in any of the human control samples, or the positive Johne’s disease sheep control samples.
“This was also the first time where the spheroplastic, or L-forms, of the bacterium have been detected and associated with human disease in tissue sections. On this basis, the results point to cell-wall deficient mycobacteria, which have been recognised for years, as the underlying cause of Crohn’s disease.”
The need for further research
“John and I are continuing research into MAP and to understand its genomic structure. Our assessment is the bacterium has a small genome and depends on host mechanisms and nutrients in the body to survive and replicate,” says Dr Tie.
“We think the findings suggest novel pathogenetic mechanisms which may lead to other diseases, such as sarcoidosis, where clusters of cells called granulomas form in various organs and the immune system cannot eliminate the invading pathogen.
“The granulomatous tissue reaction seen in Crohn’s disease cases is similar to sarcoidosis, another disease where the cause is not known, however, a recent nasal biopsy from a sarcoidosis patient also contained CWDM.”
If the link between CDWM and Crohn’s disease is confirmed, treatment could shift from managing symptoms with steroids, immunosuppressants, and surgery, to targeting the underlying infection. A similar paradigm shift occurred with gastric ulcers which went from being caused by stress and acid, to being caused by H pylori and led to a Nobel Prize.
“Current treatment focuses on controlling inflammation but greater attention should be given to developing therapies to eliminate or neutralise cell wall-deficient bacteria. While studies remain limited, the work which has been done, shows patients treated with antimycobacterial therapies have reported positive outcomes,” says Dr Tie.
“A blood test, or liquid biopsy, could also enable earlier diagnosis and reduce disease progression, scarring and the need for surgery. These bacteria can be cultured from blood and other body fluids, providing a potential pathway for earlier intervention.”
Conclusion
Dr Tie compares the potential significance of this research with the discovery of Helicobacter pylori as the cause of gastritis and peptic ulcer disease.
“Crohn’s disease is typically diagnosed only once it has become chronic and is regarded as an autoimmune disease affecting people genetically predisposed. However, most people know someone affected and understand how debilitating it can be for sufferers.
“Researchers around the world are investigating the condition, but clinical research is often difficult to advance, because pathologists and specialist clinicians face significant pressures on their time and resources. This represents a significant blind spot in modern medicine.
“However, there is a real opportunity for New Zealand researchers, supported by Awanui Labs, to contribute to a deeper understanding of Crohn’s disease.
“This research has shown a type of mycobacterium as a possible underlying cause, and provided the basis for more work, to potentially reshape the way Crohn’s disease is diagnosed and treated here and around the world.”